Synergy and Innovation: HIV and AIDS Integrated Journey
February 19, 2026Between Regulation and Action on HIV and AIDS Control
The national government policy takes a comprehensive and integrated approach in the HIV and AIDS response to achieve the Three Zero targets of no new HIV infections, no deaths due to AIDS, and no discrimination against PLHIV. However, its implementation has many challenges, especially related to cross-sector collaboration, program sustainability, and easy access and quality of services for PLHIV.
New HIV infections in Indonesia have declined over the past decade, but ending AIDS by 2030, as targeted by the government, remains challenging. The difficulty of early detection, the suboptimal quality of ARV treatment, and the persistence of stigma and discrimination are some of the obstacles in achieving zero new infections, zero AIDS-related deaths, and zero discrimination.
The World Organisation for HIV and AIDS (UNAIDS) estimates that globally, 39.9 million people are living with HIV, and by 2023, there will be 1.3 million new HIV infections. Further data shows 630,000 people died from AIDS, and 30.7 million people received ARV therapy. In the Asia and Pacific region, the number of people living with HIV reached 6.7 million, with 300,000 new infections. The death rate from AIDS reached 150,000, and the number of PLHIV receiving ARVs reached 4.5 million.
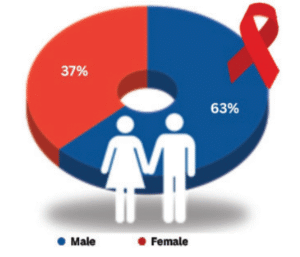
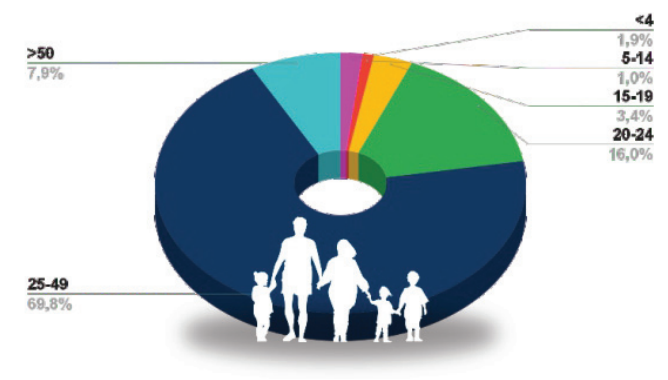
In Indonesia, the number of HIV cases was recorded at 571,637 cases, with 27,569 new HIV infections. The number of AIDS deaths reached 27,349 cases, and 217,482 ARV recipients were recorded. This data shows that despite the ongoing efforts in the HIV and AIDS response, there are still significant challenges in reducing new infections and AIDS deaths. The number of PLHIV has reached more than half a million, while new infections and mortality rates remain high. Improving access to ARV therapy is an essential step in reducing the impact of this epidemic. HIV in Indonesia is more concentrated in a few regions, with an adult HIV prevalence (>15 years) of 0.26%. Most PLHIV in Indonesia are men (63%), while women account for 37% of the total cases. PLHIV are predominantly in the 25-49 years age group (69.8%), which is the productive age population. The 20-24 year age group also has a high rate of 16%. Children and adolescents have smaller proportions, with those ≤4 years old (1.0%) and 5-14 years old (1.9%).[1]
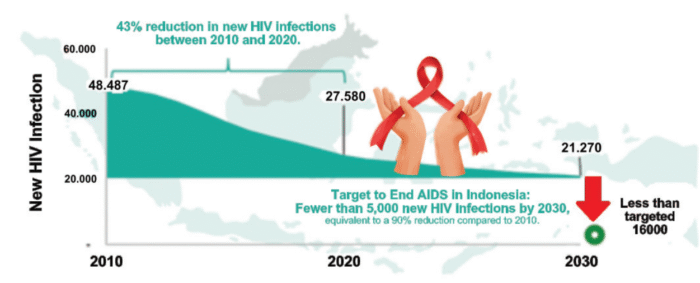
The government has set the Three Zero targets of no new HIV infections, no AIDS deaths and no discrimination against PLHIV, which it hopes to achieve by 2030. Looking at the trend, there was a 43% decrease in new HIV infections between 2010 and 2020 (from 48,487 cases in 2010 to 27,580 cases in 2020). By 2030, the number of new infections is still projected to reach 21,270 cases, exceeding the set target of below 5,000 cases. Achieving the End AIDS 2030 target still faces major challenges even though Indonesia has experienced a decline in new HIV infections in the past decade. Strengthening early detection, ARV treatment, and reducing stigma against PLHIV are key steps in achieving the Three Zero target.[2]
Indonesia’s national strategy and targets to end AIDS by 2030 align with global targets. The Indonesian Ministry of Health has developed a roadmap divided into three stages: 2022, 2025, and 2030, with a focus on reducing new HIV infections and AIDS deaths. In 2022, there is no specific target for new HIV infections, but efforts are made to strengthen case finding and treatment. The achievement indicators set are 79% of PLHIV found, 33% of PLHIV receiving ARV treatment, and 6% of PLHIV with suppressed viral load.
By 2025, the target is to reduce new HIV infections by 75% compared to 2010, from 0.21 per 1,000 population to 0.05 per 1,000 population. The achievement indicators are 89% of PLHIV found, 73% of PLHIV receiving ARV treatment, and 63% of PLHIV with suppressed viral load. By 2030, the target for new HIV infections will decrease by 90% compared to 2010, from 0.21 per 1,000 population to 0.02 per 1,000 population, and the target for AIDS deaths will also decrease by 90%, from 7 per 100,000 population to <1 per 100,000 population. The achievement indicators set are 95% of PLHIV are found, 95% of PLHIV receive ARV treatment, and 95% of PLHIV have a suppressed viral load.
As part of the global “End AIDS” target, Indonesia aims to reduce the number of new HIV infections to less than 370,000 by 2025 and AIDS deaths to less than 250,000 globally. By 2030, the number of new HIV infections and AIDS deaths will decrease by 90% compared to 2010.
This roadmap shows Indonesia’s commitment to reducing the number of new HIV infections and AIDS deaths through increased detection, ARV treatment, and viral load suppression. Achieving this target requires the cooperation of various parties, including the government, health workers, communities, and society. A viral load test is conducted to determine the amount of virus in the blood of PLHIV.[3]
The Indonesian Ministry of Health is committed to transforming the national health system by emphasising primary health care as part of the six main pillars of health transformation. Indonesia’s health system transformation targets improvements in primary healthcare, referral, health security, financing, human resources, and technology to create a stronger and more competitive health system. This commitment supports achieving a more inclusive and sustainable national health vision. This health system transformation aligns with the president’s vision to create a healthy, productive, independent, and equitable society. The primary focus of the medium-term national development plan in the health sector includes: improving maternal, child, family planning, and reproductive health; accelerating improvements in community nutrition; improving disease control; encouraging the healthy living community movement; and strengthening health systems and drug and food control. In primary care transformation, the main focus of basic health services for the community is carried out through enhancing the role of cadres; health campaigns, and digital-based community movements and community leaders; expanding immunisation coverage to 14 antigens and implementing a national disease screening program; screening 14 diseases with the highest mortality rates in each age group; preventing stunting, and improving antenantal care service (ANC); revitalising and standardising public health centre, integrated service post, community health laboratories, and home-visit services.[4]
The national strategy for HIV AIDS and STIs Response has been set by the Indonesian Ministry of Health with ambitious targets by 2030, which include: 95% of PLHIV know their status, 95% of PLHIV receive ARV therapy, and 95% of PLHIV on ARV therapy have a suppressed HIV. The response strategy to achieve these targets is divided into four main pillars: prevention, surveillance, case management, and promotion.
The prevention strategy includes the implementation of combination prevention in key populations, such as condom and lubricant use, STI screening and treatment, sterile injecting equipment, and methadone maintenance therapy; pre- and post-exposure prophylaxis to reduce the risk of transmission; prevention of mother-to-child transmission; HPV vaccine to prevent related infections; routine screening; and implementation of standard precautions in health services.
Strategies for surveillance include testing and tracing, including self and facility-based screening and Early Infant Diagnosis (EID); strengthening epidemiological surveillance, including data collection and analysis related to HIV and STIs; monitoring ARV drug resistance and gonorrhoea; and using data to support evidence-based decision-making.
Strategies for case management include standardised HIV treatment with high-quality, low-toxicity ARV therapy; prevention and treatment of sexually transmitted infections and opportunistic infections (including tuberculosis); Multi-Month Dispensing (MMD), which provides sufficient ARV drugs for several months to improve patient adherence; elimination of mother-to-child transmission of HIV, syphilis, and Hepatitis B; and treatment monitoring with regular viral load checks.
The strategies set in terms of health promotion are reproductive health education and transmission prevention through safe behaviour change campaigns; community and religious leaders’ involvement to increase public awareness; and the use of print, electronic, and social media in disseminating information related to HIV, AIDS, and STIs.
This strategy was established so that Indonesia can achieve global targets in HIV and AIDS control and realise a healthier society that is free from stigma towards PLHIV. Implementation in the field still faces various challenges, even though government policies have been comprehensively designed through Regulation of the Health Ministry Number 23 of 2022, as illustrated in the findings of the HIV and AIDS Integrated Control program conducted by CD Bethesda YAKKUM in 2022-2025.[5]
Realities of HIV and AIDS Integrated Control Programs in Belu Regency and Yogyakarta Municipality
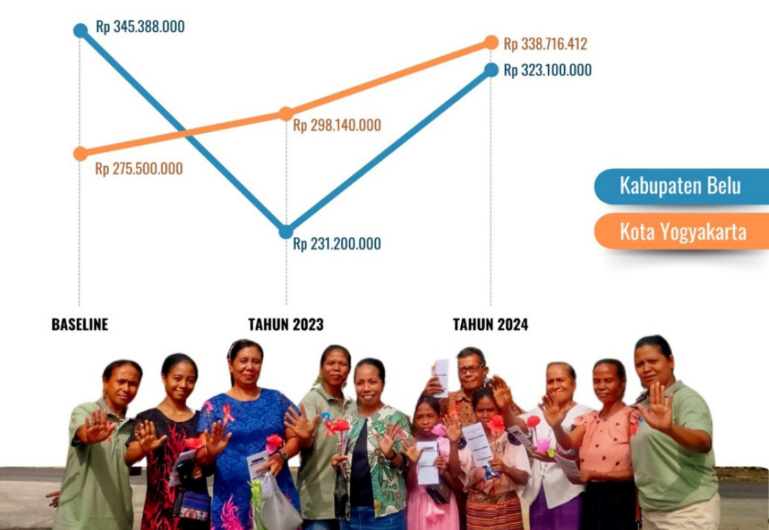
From a policy perspective, HIV and AIDS control programs have not been a top priority issue for the governments of the Belu Regency and Yogyakarta Municipality.
This can be seen from the specific budget allocation for HIV and AIDS programs, which has not increased significantly. Advocacy efforts continue to be made so local governments, through the Health Office, can integrate HIV programs into other health policies. The program also noted several supporting factors that contributed to the optimisation of HIV and AIDS control programs. For example, the District Health Office of Belu Regency utilises 90% of its budget allocation for mentoring activities that directly target PLHIV. In Yogyakarta Municipality, the integration of HIV and AIDS programs with other health issues is a strategy implemented.
The network of non-governmental organisations and concerned groups, including the PLHIV community in Yogyakarta Municipality, is essential in advocating and influencing policymakers to increase attention to the program. In Belu Regency, the involvement of peer support groups and PLHIV who have been open about their status and actively participated in socialisation in villages and sub-districts, helped increase public awareness and encouraged local government attention to the budget for PLHIV assistance.
Several constraining factors have caused the budget allocation for HIV and AIDS programs not to increase significantly. One of them is the policy of the Regent of Belu, which assumes that the free medical treatment program for citizens with ID cards of the Belu Regency already covers the needs of PLHIV. On the one hand, this policy is good enough to be able to reach all the people of Belu Regency, but on the other hand, the policy has hampered the specific budget allocation in the regional income and expenditure budget for HIV and AIDS programs. The limited budget ceiling in Belu Regency and Yogyakarta Municipality is further exacerbated by the budget priorities for the 2024 general election and the stunting program, which diverts the local government’s attention from the HIV and AIDS Control program.
The program also noted several other realities that can describe the condition of HIV and AIDS control, in addition to some supporting and inhibiting aspects related to the achievement of indicators.
Programs and Policies in Yogyakarta Municipality
The policy of dissolving the National AIDS Commission in 2017, as stipulated in Presidential Regulation Number 124 of 2016, is challenging. This policy has shifted the responsibility of coordinating the HIV and AIDS response from the National AIDS Commission to the Ministry of Health and health offices at the local level. The loss of the role of the AIDS Commission of Yogyakarta City has caused the burden of coordination to shift to the Health Office of Yogyakarta City entirely. Coordination and synchronisation of cross-sectoral programs is less than optimal because the Health Office cannot focus on only one health issue.
Although the regional action plan has been formulated with a clear division of roles among local government departments, the responsibility for implementation remains centred on the Health Office. Ideally, the regional action plan should ensure cross-sectoral involvement in HIV and AIDS control efforts, with active roles played by the Social Affairs, Education, Women’s Empowerment, Child Protection, and others. In practice, however, local government departments have not thoroughly carried out their responsibilities, leaving the Health Office to bear most of the burden of coordination and programme execution. This results in limitations to a comprehensive approach to the HIV and AIDS response, which should encompass social, economic, and educational dimensions in addition to medical ones. To improve the effectiveness of the regional action plan’s implementation, more substantial commitment from all local government departments and a more effective coordination mechanism are required, ensuring the programme operates synergistically and sustainably.[6]
The high turnover rate of health workers in Yogyakarta City also challenges the continuity of services for PLHIV. The frequent turnover of medical personnel has led to a disconnection in the flow of information and experience in dealing with PLHIV. As a result, the services provided are not always consistent with the established standards, especially in counselling, ARV treatment management, and psychosocial support. New medical personnel often have not received specialised training related to HIV and AIDS, potentially reducing service quality. A better knowledge transfer system, such as orientation programs for new health workers and increased training frequency on comprehensive services for PLHIV, is needed.
The shift of public health centre services towards integrated primary care in Yogyakarta City has resulted in significant adjustments in the HIV and AIDS service system, which previously had its clinic. Integrated primary care organises primary health care based on the life cycle, rather than by program, so the public health centre divides staff into clusters according to the life cycle and health problems experienced by patients. HIV and AIDS services that previously stood alone are now integrated into these clusters. The implementation of this approach still faces challenges, including the adjustment of the HIV and AIDS service system that was previously based on separate clinics. Collaborative efforts between health workers and relevant stakeholders are needed to ensure HIV and AIDS services remain optimal within the integrated primary care framework.[7]
ARV drug distribution in Yogyakarta City is relatively stable, ensuring drug availability for PLHIV on therapy. Further evaluation is still needed to identify constraints in the supply chain and patient access. Some factors that need to be reviewed include stock sustainability at health facilities and possible administrative or logistical barriers that may affect distribution. It is essential to ensure that PLHIV not only receives ARVs regularly but also has access to adequate information and assistance to improve treatment adherence. This evaluation will help strengthen the ARV distribution system to be more responsive to the needs of PLHIV and support efforts to achieve HIV and AIDS control targets in Yogyakarta City.
Programs and Policies in Belu Regency
In the Belu Regency, the number of health services implementing the continuum of care by the Ministry of Health standards has increased. The program noted that by the second year, the addition of 4 health centres and one hospital in Belu Regency that implemented the HIV-continuum of care service is evidence of the success of advocacy conducted with peer support groups and the AIDS care community to bring services closer to PLHIV.
The success of this program is supported by the active role of the Health Office in Belu Regency in increasing the number of service facilities that implement HIV-continuum of care service and ensuring improved service quality through the development of PLHIV-friendly monitoring tools. However, the program still faces challenges. One is the movement of trained health workers in the Belu Regency to other facilities, while the replacement officers have not received HIV training. The limited number of psychologists in the Belu Regency also poses a challenge to access to psychosocial support for PLHIV.
Another challenge faced in the Belu Regency is the implementation of care and support, especially in human resources and service capacity. The limited number of health workers with specialised expertise in HIV and AIDS is a significant challenge, especially in areas with limited access to training and competency development. Service capacity at health centres still needs to be improved to provide comprehensive services for PLHIV, including counselling, monitoring adherence to ARV therapy, and early detection of opportunistic infections. Addressing this requires increasing the number and competence of health workers through continuous training, optimising the referral system to better-equipped health facilities, and policy support that ensures effective and sustainable CST services.
The lack of frequent training for CST teams in the Belu Regency directly impacts the implementation of the HIV continuum of care service. CST teams play a critical role in ensuring that PLHIV receives quality care, adequate psychosocial support, and continued access to ARV treatment. Lack of training, health workers, and caregivers often leads to difficulties in adopting the latest guidelines, addressing the psychological and social challenges of PLHIV, and providing appropriate education on medication adherence. Lack of capacity updates can also lead to inconsistencies in services and reduced effectiveness of mentoring. Increasing the frequency and quality of training for CST teams is a strategic step that needs to be strengthened to optimise services and meet the needs of PLHIV.[8]
The coverage of HIV and AIDS services in Belu Regency is still lower than in other regions, with the number of PLHIV found and started on treatment still far from the national target. Limited access to health services, lack of trained medical personnel, and strong social stigma are the main factors that hinder early detection and continuation of treatment for PLHIV. Many PLHIV are still undiagnosed or reluctant to start ARV therapy due to various obstacles, including fear of discrimination. More proactive strategies are needed, such as strengthening the referral system, improving community education, and expanding access to HIV and AIDS services at the health centre level to make it more accessible to key populations and the general public.
Access to ARV and viral load testing services in Belu Regency remains suboptimal, primarily due to geographical and logistical constraints. As a region with challenging terrain, including remote areas and limited transportation access, PLHIV often faces difficulties in obtaining routine ARV treatment directly. Despite two years of programme implementation aimed at expanding CST services at the public health centre level, some PLHIV continue to encounter problems. This is partly due to family discrimination, making the role of the public health centre’s HIV programme manager and peer support groups particularly vital in ensuring timely access to medication and promoting treatment adherence.
The limited viral load testing facilities in this area make it difficult for PLHIV to monitor the effectiveness of ARV therapy regularly, which risks reducing treatment success. Viral load testing can only be done at the Regional Public Hospital of Atambua, so PLHIV who live far from the hospital often experience problems. The program has facilitated capacity building for community health centre staff to be able to refer specimens for viral load testing, which hopefully will help PLHIV to access this test more easily.
Conclusion
Based on the above description, it can be concluded that the national policy has led to a comprehensive and integrated approach in the HIV and AIDS response. The reality on the ground shows that there are still many challenges in implementation, especially related to cross-sector collaboration, program sustainability, and access to services for PLHIV. Efforts are needed to strengthen the coordination system, increase the capacity of health workers, and promote broader involvement of communities and NGOs to ensure that the policy can be run according to expectations and targets set.
Ghanis Kristia
References:
[1] Ma’ruf, A. (2024). Policies and Strategies for HIV Prevention in Indonesia. Jakarta: Ministry of Health of the Republic of Indonesia.
[2] Ma’ruf, A. (2024). Policies and Strategies for HIV Prevention in Indonesia. Jakarta: Ministry of Health of the Republic of Indonesia.
[3] KNCV Indonesia Foundation. (2023). The Importance of HIV Viral Load Testing. https://ayosehat.kemkes.go.id/
[4] Ma’ruf, A. (2024). Policies and Strategies for HIV Prevention in Indonesia. Jakarta: Ministry of Health of the Republic of Indonesia.
[5] Ma’ruf, A. (2024). Policies and Strategies for HIV Prevention in Indonesia. Jakarta: Ministry of Health of the Republic of Indonesia.
[6] Yogyakarta City Health Office. (2022). Development of Regional Strategies and Action Plans for HIV/AIDS Prevention in Yogyakarta City for 2022. https://kesehatan.jogjakota.go.id
[7] Sudiana, S. (2024). Primary Care Integration (ILP) in Community Health Centres: a Public Health Perspective. Website Birokrat Menulis
[8] Mujiati, Pardosi, J.F., & Syaripuddin, M. (2015). Evaluation of the Implementation of HIV-AIDS Care, Support, and Treatment (PDP) Service in West Java and Papua in 2012. Indonesian Journal reproductive Health, 5(2).


{kind=link}
{kind=link}