Collaboration and Creativity: Key to Overcoming Healthcare Disparities
Disparities in HIV-related health services in Indonesia remain evident from one region to another in terms of geographic accessibility, service quality, availability of trained health workers, and barriers due to stigma. These disparities impact access to HIV testing, treatment, and support services for vulnerable groups. Health workers must be creative in adapting to the challenges in their service areas.
Indonesia has developed an extensive health infrastructure to address HIV and AIDS, with services available at various levels, including public health centres and hospitals. By 2023, around 10,180 primary health centres across Indonesia will provide comprehensive primary health care services. The number of facilities providing HIV testing and antiretroviral (ARV) has also increased significantly, with almost two-thirds of ARV providers being health centres. However, challenges such as stigma, discrimination, and accessibility issues still prevent many PLHIV from accessing friendly and inclusive health services.
Yogyakarta City (32.5 km²) has established a network of health facilities that can be categorised as comprehensive services to address HIV and AIDS. These health services aim to provide accessible and quality services for those affected. Although in planning, the health services in Yogyakarta continue to adapt to new systems and policies from the government, in practice, there are still challenges and barriers, or even criticisms raised by those who access the services. Before discussing this further, let us first look at the general picture of health facilities and services in Yogyakarta City.
Based on 2023 data, 18 health centres in Yogyakarta City are equipped with adequate facilities to manage HIV and AIDS cases. The public health centres in Gedongtengen, Tegalrejo, Mantrijeron, Umbulharjo I and II, Pakualaman, Danurejan I and II, Gondomanan, Jetis, Ngampilan, Kraton, Wirobrajan, and Mergangsan have been designated by the Yogyakarta City Health Office as Care, Support, and Treatment (CST) service providers. In contrast, the public health centres in Kotagede I, Kotagede II, and Gondokusuman I and II have not yet begun offering HIV and AIDS care and treatment services, as no cases have been reported in their respective areas.
In addition to public health centres, several hospitals support HIV treatment and assistance in Yogyakarta. These hospitals include Bethesda, PKU Muhammadiyah Yogyakarta Hospital, Panti Rapih Hospital, Yogyakarta City Hospital, Pratama Hospital, and DKT Dr. Soetarto Hospital.
As for the Belu Regency with a vast area of 1,284.94 km², health service providers in the Belu Regency have also developed various efforts to address HIV and AIDS challenges through improved health services and community collaboration. As of March 2023, the Belu Regency Health Office conducted an initial survey and noted that 17 health centres serve the Belu Regency. Six public health centres already have CST service: Umanen, South Atambua, Silawan, Atapupu, Wedomu, and Haekesak. The other 11 health centres are Webora, Rafea, Halilulik, Ainiba, Haliwen, Laktulus, Atambua City, Aululik, Weluli, Dilumil, and Nualain. In addition to health centres, Belu Regency is assisted by two hospitals accepting PLHIV for treatment and assistance services. Regional Public Hospital Atambua, a government-owned regional general hospital, is located in Atambua City, and Marianum Halilulik Catholic Hospital, a private hospital in West Tasifeto District.

Challenges and Opportunities in HIV Control: a Health Services Perspective
Progress and Changes
CD Bethesda YAKKUM in 2022–2025 assists four puskesmas and two hospitals in Yogyakarta City with the following details: Public health centres of Gedongtengen, Umbulharjo I, Tegalrejo, and Mantrijeron, Bethesda Hospital, and Yogyakarta Regional Public Hospital. As for Belu Regency, CD Bethesda YAKKUM assisted seven health centres and two hospitals with the following details: Public health centres of Umanen, South Atambua, Halilulik, Ainiba, Silawan, Atapupu, Wedomu, Regional Public Hospital of Atambua, and Marianum Catholic Hospital.
During the mentoring and intervention period, 12 out of 15 health services have implemented the continuum of care service system by the Indonesian Ministry of Health standards. Continuum of care is a health care system designed to address HIV infection in a comprehensive, integrated, and sustainable manner, from prevention to treatment, according to the Indonesian Ministry of Health standards. In practice, before a service can be categorised as a continuum of care service, it must undergo training organised by the Indonesian Ministry of Health and implement HIV Care and HIV CST.
Achievements and Changes in Health Services in Yogyakarta City:
- Three out of six CD Bethesda YAKKUM partner providers in Yogyakarta have opened and implemented pre-exposure prophylaxis services, also known as PrEP. PrEP is a treatment service (in the form of pills or injections) that can be accessed by people at risk of HIV to prevent the spread of the virus.
- Each HIV and AIDS service provider in Yogyakarta Municipality has a psychologist who can be accessed at any time by PLHIV for counselling purposes when accessing HIV and AIDS services/treatment.
- Communication is well maintained through WhatsApp messages and there is regular feedback, both positive and negative, provided by PLHIV in each service either directly or through messages.
- The public health centre of Gedongtengen and Umbulharjo received viral load machines from the province. As of April 2024, there is also an MoU. This machine will be used in May 2024. However, the quota is not much because the reagents given are only 40, whereas more than 300 PLHIV need them. Although a data validation meeting was held, there was an input that it is possible that other PLHIV can also conduct viral load tests through referrals. The MoU did not mention the continuity of stock from the centre.
- Tegalrejo Public Health Centre applies a comprehensive policy approach. This means that if there is a new policy, the security guards and cleaning team will be involved to understand the new policy. For example, registration and other service personnel in the HIV program understand what it means to be PLHIV-friendly and inclusive. However, the security guards are uninvolved, so they are still cold to PLHIV and do not reinforce the new policy. This is also implemented to handle complaints from patients or prospective patients.
- Services in the Belu Regency have also made steady progress in completing the continuum of care service to the Republic of Indonesia’s Ministry of Health standards. In the approximately eight months since the survey was completed in 2023, there have been changes in each service. The Public Health Centre of South Atambua and Halilulik have completed the Republic of Indonesia’s Ministry of Health standards. As for ARV therapy, all health centres and hospitals have provided the service, although with a note, some health centres, such as the Public Health Centre of Silawan and Ainiba, still use the referral system for ARV services.
- Ahievements and Changes in Belu Regency Health Services:
- There has been progress in the seven CD Bethesda YAKKUM partner public health centre services. PLHIV who access ARVs at the puskesmas or through the public health centre have taken the initiative to have a viral load test as part of comprehensive treatment.
- An AIDS Care Community has been established in the Halilulik Health Centre service area that can help health services to reach PLHIV.
- Partner public health centers have collaborated with AIDS care communities and peer support groups to address LFU. Public Health Centre of South Atambua managed to reduce the number of LFU from 11 PLHIV to 9 PLHIV.
- In 2024, there was also an increase in PLHIV taking their own medication at the public health centre that serve the CST service.
- Partner health centres have routinely and regularly conducted mobile VCT testing in health centre service areas in the Belu Regency. Umanen Health Centre has successfully conducted outreach and HIV testing to high-risk groups such as female sex workers.
- Marianum Halilulik Hospital, as a Catholic-based hospital, involves spiritual support and spiritual guidance for PLHIV accessing ARVs at the hospital.
- After synchronising data between the Belu Regency Health Office and the Regional Public Hospital of Atambua, the total number of PLHIV until 2024 is 578; 324 are on ARVs, 44 are on LFU, 84 have died, and 126 are other.
Stigma and Health Service
Several sociologists worldwide define stigma as a dynamic process of devaluation that significantly discredits an individual in the eyes of others. ³Stigma is an attribute that can make individuals lose confidence and can be a scary thing.⁴ Based on the Indonesian Dictionary, stigma is defined as a negative characteristic attached to a person due to the influence of their environment. Based on some of the definitions above, it is clear that stigma is closely related to the environment and how a person’s way of viewing the world. Despite having different backgrounds, there will still be one pattern that is lived together in a society, and that is how negative stigma, especially on PLHIV, works.
In practice during 2023-2024, there were still PLHIV who complained of various offensive and stigmatising treatments by health workers. The treatment ranged from minor ones, such as intimidating glances, to judgmental statements. Although this may be considered a sentimental factor by some, in reality, it can demoralise PLHIV, making them reluctant or lazy to seek treatment. Stigma can prevent a person from seeking necessary health services, support, or disclosure of their status for fear of negative consequences. There is even a phenomenon of double stigma among PLHIV in Yogyakarta City, where PLHIV with disabilities often face double stigma, namely the stigma associated with HIV and the stigma associated with their disability. This can lead to social isolation and discrimination in various places, including health services. Stigma does not mean simply mistreating PLHIV through violence and words. When the health care system or people deliberately ignore the needs of PLHIV, it is also considered stigma.
The high need for stigma reduction in health services has led CD Bethesda YAKKUM and health services in Yogyakarta and Belu to develop an inclusive monitoring system. The monitoring system seeks to guarantee and ensure that PLHIV and people who access HIV information, treatment, and assistance can get services that are non-discriminatory, friendly, and inclusive.
In 2024, a series of PLHIV-friendly monitoring tools developed jointly by the Yogyakarta City Health Office and CD Bethesda YAKKUM were implemented by four health centres and two hospitals in Yogyakarta City. Meanwhile, for the Belu Regency, it will only be conducted in mid-2025. The following is a brief overview of the results of the PLHIV-friendly monitoring in Yogyakarta City:
*4 is the highest score and 1 is the lowest score.
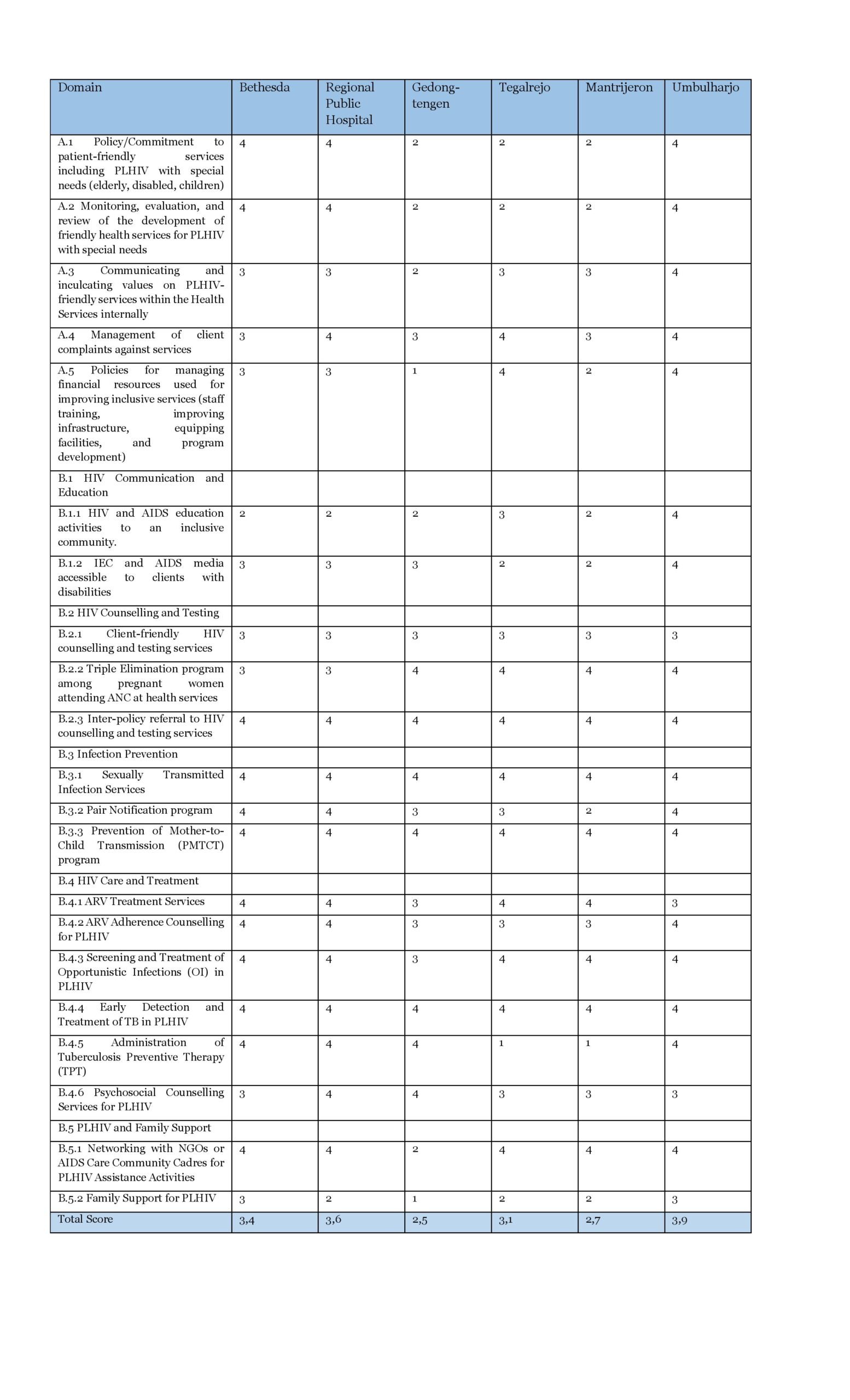
The assessment system for this tools includes two main categories, namely Governance and Management Practices. Management practice are further divided into five categories, namely HIV Communication and Education, HIV Counselling and Testing, Infection Prevention, HIV Care and Treatment, and Support for PLHIV and Families. The score range is set from 1 to 4. The assessment of each category is adjusted according to this score. The Governance Aspect consists of patient-friendly service policies/commitments, monitoring and evaluation, communication and instilling service values in the PLHIV domain, patient complaint management systems, and financial resource management.
The assessment results for six service locations in Yogyakarta City showed that the score for governance was almost perfect at 3.9, or 96.9%. Each service already has an adequate and robust system based on its respective category.
In terms of the Management Practices aspect of the service, the scores of each service tended to be more diverse, because the management practices aspect also includes various categories. The average score shown in the intervention services was 3.3 or 82.5%. The score for providing Screening and Treatment of Opportunistic Infections (OI) in PLHIV reached the highest in domain 3.8.
Generally, the quality of services based on the monitoring and evaluation tools of PLHIV-friendly tools monitoring is satisfactory. The average score or service achievement touched 3.6 or 83.60% of the maximum score of 4 or 100%. Based on data collected through FGDs, even if a service does not fulfil a category in the monitoring tool, they are actively working to achieve that category.
The relationship between stigma and healthcare facilities is complex and significant. Stigma within healthcare facilities or services can significantly reduce access, quality of care, and health outcomes for affected individuals. Addressing stigma through education, policy change, and improved relationships between patients and healthcare providers is critical to creating a more inclusive and effective healthcare system.
Service Gaps as Barriers
HIV-related health service disparities in Indonesia are still evident in some regions. These include geographic accessibility, quality of care, availability of trained health workers, and stigma-related barriers. These disparities inevitably impact PLHIV’s access to testing, treatment, and support services.
Service gaps are caused by several factors that may not be immediately reversible. In comparison, Yogyakarta City’s intervention area of 32.5 km², consisting of 14 sub-districts, 45 villages, is served by 18 community health centres and 12 public hospitals. Meanwhile, Belu Regency, which covers 1,284.94 km², is divided into 12 sub-districts, 12 villages, and 69 villages. It is served by only 17 community health centres and four hospitals until 2023. Geographically, it can be seen that comparing health services in Belu Regency and Yogyakarta City is not an equal comparison. This reality is certainly not something that can be changed in a matter of years. Therefore, the government and the community must collaborate, adapt, and innovate to close this systemic gap.
Gap Effect
Based on observations and experiences with the intervention areas in Belu Regency and Yogyakarta Municipality, the following are some of the effects of gaps in the integrated HIV control process in 2022-2025:
1. ARV Availability and Completion of Treatment
Through observations and interviews with health workers in Yogyakarta City, ARV shortages rarely occurred, except at the beginning of the COVID-19 pandemic, in 2020. Meanwhile, the Regional Public Hospital of Atambua, as the centre of HIV services in Belu Regency, still often experiences shortages of ARV drugs because many PLHIV prefer to take ARVs at the regional public hospital rather than at health centres that have CST service. Many PLHIV do not want to access ARVs at the CST service in health centres that are closer to their residence due to the fear of being ‘found out’ by neighbours or health workers who know PLHIV personally. This resulted in heavy traffic of ARV collection services at the Regional Public Hospital of Atambua and overwhelmed the health workers. Meanwhile, in the case of Yogyakarta City, many PLHIV still take ARVs at more distant services even though CST services are closer due to convenience reasons. The availability of ARVs in the Belu Regency itself is still highly dependent on the smooth distribution from the East Nusa Tenggara Provincial Health Office. The communication flow is often not soft, causing delays in drug stock.
2. Lack of CD4 and viral load testing equipment
Lack of CD4 and viral load testing equipment. Until mid-2024, not all health centres and hospitals in Belu Regency could conduct CD4 count and viral load tests, so patients had to visit specialised hospitals. Even the Regional Public Hospital of Atambua, which provides viral load and CD4 testing services, has to send samples to a hospital with an adequate laboratory in Kupang. This will slow down the process and discourage many PLHIV due to the perceived complexity of the process. As for Yogyakarta City, each health centre with CST service can take samples and send them to the two hospitals in Yogyakarta City, namely Sardjito and Panti Rapih.
3. Limited number of trained health workers
Health facilities in Indonesia’s outermost regions, in general, often lack doctors, nurses, and counsellors trained in HIV and AIDS response. Even in the Belu Regency, several services have implemented the CST, but still have personnel who have not received training. This happened because the health workers had to replace the CST-trained personnel who had moved to other locations. There are also cases where some general practitioners are not adequately trained in HIV care, leading to misdiagnosis or reluctance to treat PLHIV. This is detrimental as PLHIV may miss the opportunity for early detection and fall ill. In Yogyakarta City, there are still doctors who are reluctant to treat pregnant women with HIV because they do not understand the concept of Prevention of Mother to Child Transmission (PMTCT). In the Belu Regency, no psychologist is available for PLHIV, while Yogyakarta City has at least one psychologist for each service.
In addition to CST training, health workers in HIV services should also receive more in-depth anti-stigma service training. Several health workers at community health centres in Yogyakarta City reported that they also train security guards to ensure that PLHIV feel welcome when they first set foot in the service. This is important for each service to think about, as the more welcoming and inclusive an HIV service is, the higher the chance of reaching high-risk groups, especially those who face more stigma and barriers, such as LGBTQ+ populations, sex workers, and people who use drugs. These populations are vulnerable to discriminatory attitudes from health providers, making them reluctant to seek treatment. Finally, in the Belu Regency, health workers who oversee HIV programs struggle to provide adequate care due to the high prevalence disproportionate to the number of health workers.
4. Economic Level
Economic disparities significantly affect access to HIV treatment, especially in low-income communities. A more common issue related to geographic and economic inequality is transport. Larger cities in Java, such as Yogyakarta, generally have more comprehensive HIV services, including VCT, ARVs, and HIV-specific clinics that are more widespread throughout the city. In rural and remote areas such as the Belu Regency, health facilities are limited and centred on one or two services. The real effect felt by PLHIV in the Belu Regency is that although access to ARVs is free, they still have to spend a significant amount of money on transport costs to reach health services. Individuals with limited financial resources find it difficult to pay for transport costs and other costs to support PLHIV treatment, such as costs for vitamins and additional supporting food.
Improvement Efforts
To address the issues created by the disparities in HIV service provision, services must be more creative and adaptable to the challenges they face.
The distance gap in Belu Regency, for example, is addressed through collaboration with the AIDS care community so that health workers can reach PLHIV who cannot afford to come to services. This ensures that PLHIV do not become LFU. The following are some steps developed by CD Bethesda YAKKUM and communities in Belu Regency and Yogyakarta Municipality to bridge the gap:
- Encourage and advocate for more HIV services to become a continuum-of-care standardized.
- Strengthen the dialogue with the local health office to ensure consistent availability of ARV drugs throughout the intervention area.
- Training more health workers: in collaboration with the Health Office, CD Bethesda YAKKUM continues to provide HIV care and stigma reduction training for doctors, nurses, and midwives.
- Reducing stigma in healthcare: implementing anti-discrimination policies in hospitals and health centers.
- With AIDS care communities and peer support groups strengthen community-based support.
[1]Statista, 2023. Number of community health centers in Indonesia from 2014 to 2023. Diambil dari https://www.statista.com/statistics/605371/number-of-community-health- centers-in-indonesia/. Diakses pada 08 Maret 2025 – 19:20 WIB.
[2]Warta Jogjakota. (2023). Upaya Kota Yogyakarta dalam Pengendalian HIV/AIDS. Diambil dari https://warta.jogjakota.go.id/detail/index/25708. Diakes pada 02 Maret 2025 – 19:35 WIB
[3]Sengupta, S., Banks, B., Jonas, D., Miles, M. S., & Smith, G. C. (2011). HIV interventions to reduce HIV/AIDS stigma: A systematic review. AIDS and Behavior, 15(6), 1075–1087.
[4]Genberg, B. L., Kawichai, S., Chingono, A., Sendah, M., Chariyalertsak, S., Konda, K. A., & Celentano, D. D. (2008). Assessing HIV/AIDS stigma and discrimination in developing countries. AIDS and Behavior, 12(5), 772–780.
[5]Badan Pemeriksa Keuangan (BPK) RI. (n.d.). Kabupaten Belu. Diakses dari https://ntt.bpk.go.id/kabupaten-belu


{kind=link}
{kind=link}